What that post does not look into is whether strength exercise, performed at the anaerobic range, increases nitrogen balance. If it did, it may lead to a counterintuitive effect: strength exercise, when practiced at a certain level of intensity, might enable individuals in calorie deficit to retain their muscle, and lose primarily body fat. That is, strength exercise might push the body into burning more body fat and less muscle than it would normally do under calorie deficit conditions.

(Strength exercise combined with a small calorie deficit may be one of the best approaches for body fat loss in women. Photo source: complete-strength-training.com)
Under calorie deficit people normally lose both body fat and muscle to meet caloric needs. About 25 percent of lean body mass is lost in sedentary individuals, and 33 percent or more in individuals performing endurance exercise. I suspect that strength exercise has the potential to either bring this percentage down to zero, or to even lead to muscle gain if the calorie deficit is very small. One of the reasons is the data summarized on this post.
Two other reasons are related to what happens with children, and the variation in spontaneous hunger up-regulation in response to various types of exercise. The first reason can be summarized as this: it is very rare for children to be in negative nitrogen balance (Brooks et al., 2005); even when they are under some, not extreme, calorie deficit. It is rare for children to be in negative nitrogen balance even when their daily consumption of protein is below 0.5 g per kg of body weight.
This suggests that, when children are in calorie deficit, they tend to hold on to protein stores (which are critical for growth), and shift their energy consumption to fat more easily than adults. The reason is that developmental growth powerfully stimulates protein synthesis. This leads to a hormonal mix that causes the body to be in anabolic state, even when other forces (e.g., calorie deficit, low protein intake) are pushing it into a catabolic state. In a sense, the tissues of children are always hungry for their building blocks, and they do not let go of them very easily.
The second reason is an interesting variation in the patterns of spontaneous hunger up-regulation in various athletes. The increase in hunger is generally lower for strength than endurance activities. The spontaneous increase for bodybuilders is among the lowest. Since being in a catabolic state tends to have a strong effect on hunger, increasing it significantly, these patterns suggest that strength exercise may actually contribute to placing one in an anabolic state. The duration of this effect is approximately 48 h. Some increase in hunger is expected, because of the increased calorie expenditure during and after strength exercise, but that is counterbalanced somewhat by the start of an anabolic state.
What is going on, and what does this mean for you?
One way to understand what is happening here is to think in terms of compensatory adaptation. Strength exercise, if done properly, tells the body that it needs more muscle protein. Calorie deficit, as long as it is short-term, tells the body that food supply is limited. The body’s short-term response is to keep muscle as much as possible, and use body fat to the largest extent possible to supply the body’s energy needs.
If the right stimuli are supplied in a cyclical manner, no long-term adaptations (e.g., lowered metabolism) will be “perceived” as necessary by the body. Let us consider a 2-day cycle where one does strength exercise on the first day, and rests on the second. A surplus of protein and calories on the first day would lead to both muscle and body fat gain. A deficit on the second day would lead to body fat loss, but not to muscle loss, as long as the deficit is not too extreme. Since only body fat is being lost, more is lost on the second day than on the first.
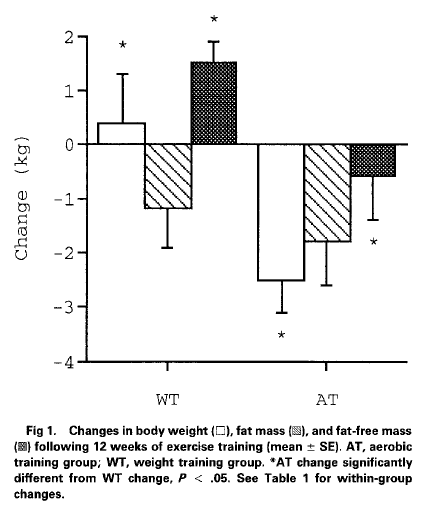
In this way, one can gain muscle and lose body fat at the same time, which is what seems to have happened with the participants of the Ballor et al. (1996) study. Or, one can keep muscle (not gaining any) and lose more body fat, with a slightly higher calorie deficit. If the calorie deficit is too high, one will enter negative nitrogen balance and lose both muscle and body fat, as often happens with natural bodybuilders in the pre-tournament “cutting” phase.
In a sense, the increase in protein synthesis stimulated by strength exercise is analogous to, although much less strong than, the increase in protein synthesis stimulated by the growth process in children.
References
Ballor, D.L., Harvey-Berino, J.R., Ades, P.A., Cryan, J., & Calles-Escandon, J. (1996). Contrasting effects of resistance and aerobic training on body composition and metabolism after diet-induced weight loss. Metabolism, 45(2), 179-183.
Brooks, G.A., Fahey, T.D., & Baldwin, K.M. (2005). Exercise physiology: Human bioenergetics and its applications. Boston, MA: McGraw-Hill.










{kind=link}